Do not turn a blind eye to bleeding, you may have to pay a King’s Ransom
Whenever there is an injury or cut, it bleeds. Bleeding stops after sometime. That’s normal. But when bleeding continues for a prolonged time, it may be abnormal. One needs to pay attention to it. One may be suffering from some inherited bleeding disorder which can cost the life due to excessive blood loss or haemorrhage following an accident, surgery or child birth. According to a report published, severe trauma results in 5 million deaths annually. At least 20% of severely injured patients are already coagulopathic upon arrival in the emergency room, means suffering from some form of bleeding disorders, may be acquired or inherited. But awareness of this problem is low, leading to late recognition and delayed treatment of coagulopathy.
Inherited bleeding disorders are rare in general population, but the total number of cases diagnosed is actually less than the actual number cases prevalent in the population. Many times it becomes apparent post-operatively. Despite the worldwide prevalence of rare bleeding disorders, knowledge of this conditions and their management is suboptimal; health care professionals often have little diagnostic and therapeutic experience with variable access to diagnostic modalities required for accurate identification. Therefore, patients often experience morbidity and mortality due to delayed diagnosis. You can assess the gravity of the problem by looking into the actual numbers of available facilities for diagnosing these disorders in our state Odisha. We have less than 10 centres that are performing special coagulation testing like factor VIII or IX assay. We have less than 5 centres that are performing von Willebrand factor assay. We have 2 odd centres who are doing inhibitor assay for haemophilia patients. We have only one centre that is performing platelet function test. There is lack of awareness among the general population about different bleeding disorders and when to seek medical advice. Secondly lack of diagnostic facility for bleeding disorder makes the situation worse. Many patients have to travel outside state to different central institutions for diagnosis and treatment. The cost of travel, stay and regular treatment at a far off place is prohibitor for many patients suffering from bleeding. Let’s understand it more.
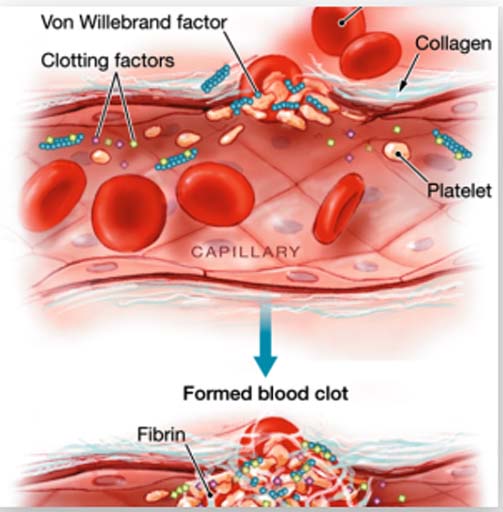

The normal process to keep the blood in fluid state and form a clot to stop bleeding at the site of injury is known as haemostasis. The blood vessel, platelets, and different proteins called as coagulation factors help in haemostasis. Prolonged bleeding will occur due to any abnormality of blood vessels or deficiency in the number or function of platelets and / or coagulation factors. The most common inherited bleeding disorders are haemophilia A due to FVIII deficiency which can affect 1 in 5000 males and von Willebrand disease (vWD) which can affect 1% of the population. Factor IX deficiency causes haemophilia B. Bleeding disorders may have variable presentations. It may include nose bleed, red to bluish patches on the skin, mouth, swelling of joints, excessive bleeding from umbilical cord, spontaneous swelling below the skin, excessive bleeding from cut, dental extraction, child birth or surgeries, heavy menstrual cycles etc. An early age of presentation with repeated similar history of bleeding manifestations indicate a possible bleeding disorder of genetic origin. If similar history has been noted in the family members then there is a high probability of inherited bleeding disorder.
Bleeding disorders can be of three types based on their presentation. Mild bleeding disorders may not present with spontaneous bleeding or bleeding with minor trauma or trivial injury. But there may be life threatening bleeding following major trauma, surgery or child birth. Severe bleeding disorders may present with bleeding manifestation from an early age and have multiple episodes. They may have bleeding manifestation to trivial trauma. Sometimes the bleeding is so severe requiring blood transfusion, or surgical suturing etc. But whatever may be the nature, we cannot take bleeding disorders lightly whether mild or severe. We need to remember even a mild bleeding disorder may present with severe bleeding during surgery or trauma costing precious life. A positive family history may be a sufficient reason to screen for it at an early age to avoid any serious consequences. Because a known foe is better than an unknown friend.

Anything that bleeds is a bleeding disorder! No. It’s a myth. Many times bleeding is acquired in nature and mostly local in nature. Inherited bleeding disorders are rare in nature. A black stool may indicate gastrointestinal bleeding. A bleed while coughing may be because of some respiratory cause. Blood in urine may be related to kidney related abnormality, stone in urinary tract, or a tumour in the bladder etc. So, patients presenting with bleeding from one site with a late age of onset are usually suffering from some other disease leading to bleeding manifestation.
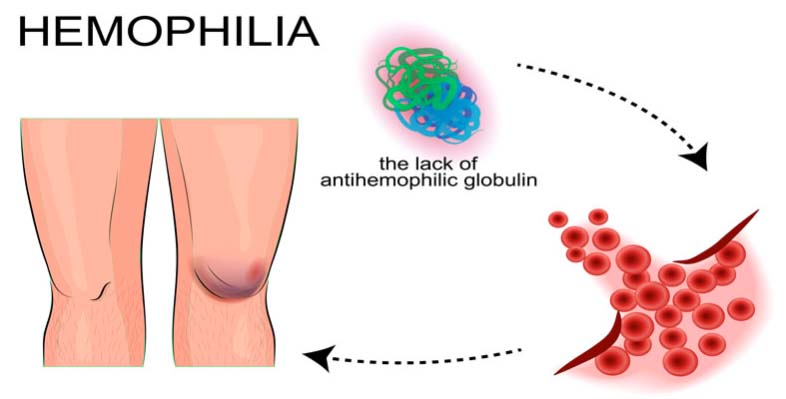
But we must be aware of certain seminal facts about the bleeding disorders. A heavy menstrual bleeding can be due to inherited bleeding disorders like von Willebrand disease or some platelet functional disorders. But majority of patients may not have an inherited bleeding disorder. But all patients with heavy menstrual bleed without a definite cause being identified should be evaluated for bleeding disorders. Do you know that a habitual abortion can indicate bleeding disorders?All patients with history of repeated abortion should be evaluated for bleeding disorder too, because factor XIII deficiency and afibrinogenemia presents as repeated abortion. Even patients with history of delayed wound healing since childhood, delayed bleeding from wound, umbilical cord bleeding or delay in healing of umbilical cord should be evaluated for factor XIII or fibrinogen tests. Many times a childhood joint swelling can be misdiagnosed as arthritis which is actually a joint bleeding and the child may be suffering from hemophilia A, hemophilia B or severe type of von Willebrand disease. One should not neglect as repeated bleeding leads to swelling of joints and in long run can lead to deformity.
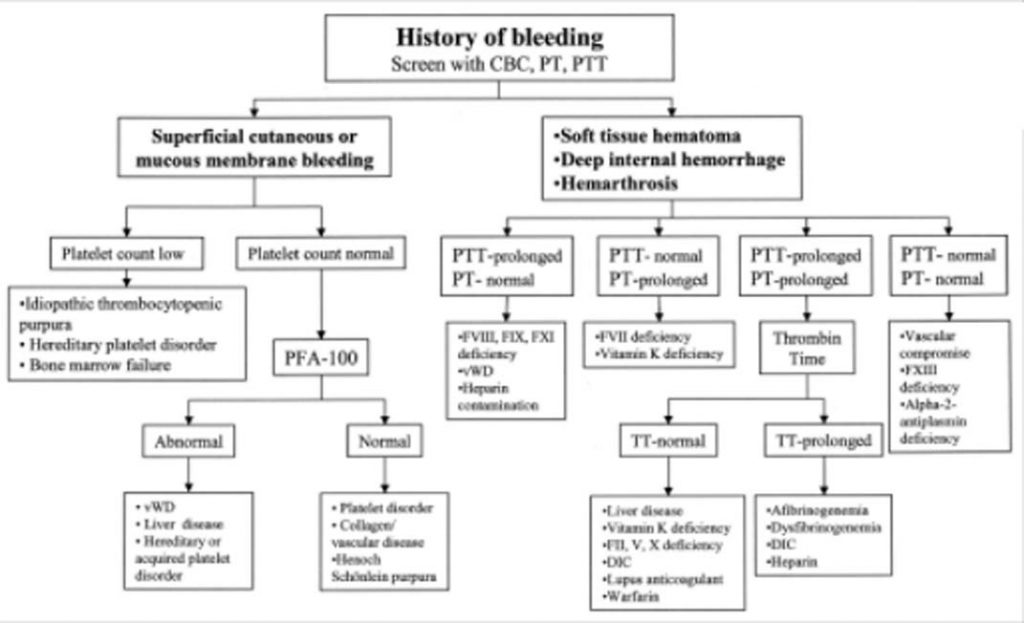
These bleeding disordersare diagnosed based on a battery of tests which include basic screening tests like bleeding time, clotting time, prothrombin time, activated partial thromboplastin time, platelet counts and morphology to highly specialized tests like specific factor assay, platelet function tests, von Willebrand factor assay, molecular studies etc. The most commonly performed tests are bleeding time and clotting time (BT & CT). But we need to know that a normal BT & CT can’t exclude all types of bleeding disorder. One cannot neglect the subjective and methodological variations involved in BT & CT and its drawback being highly error prone. A good history of bleeding, positive family history, platelet count, PT, aPTT can be the best way to screen for bleeding disorder and are widely available in many centres across the state. One found to be screen positive for bleeding disorder can be referred to higher centres for a definitive diagnosis.
The bigger question remains – Can inherited bleeding disorder be cured? Research is going on to get cure for these disorders. But in current scenario, there is no definite cure available as it involves an abnormality of the gene. But different treatment modalities are available like factor replacement therapy which can treat bleeding manifestation and avoid any life threatening events. Even prophylactic therapies are available. The treatment may be expensive sometimes. Many global NGOs like World federation of haemophilia (WFH) are committed to bring society who is involved in helping patients. The tertiary care centres in the states including medical colleges are also actively engaged in treating these special cases.We should realize that with currently available treatments, hemophilia or vWD patients can have a near normal life.
It’s a sincere request to all, let’s get aware of any abnormal bleeding, get screened and diagnosed before it’s too late which can cost more than a king’s ransom.
In concluding remark, I would like to quote from Charles Dickens’ A tale of two cities, 1859:
“It was the best of times, it was the worst of times, it was the age of wisdom, it was the age of foolishness, it was the epoch of belief, it was the epoch of incredulity, it was the season of Light, it was the season of Darkness, it was the spring of hope, it was the winter of despair, we had everything before us, we had nothing before us, we were all going direct to Heaven, we were all going direct the other way.”
The author is Associate Professor & Consultant Haematopathologists trained in CMC, Vellore and works at IMS & SUM Hospital, Bhubaneswar